Graphic: A pregnant woman lies on a hospital bed. A smiling female in a RFDS polo shirt holds a doppler over her pregnant tummy. They are both smiling.
Shared Care between RFDS Midwives, Doctors and tertiary hospitals provide the finest care for pregnant women living in rural and remote areas.
Research reveals that geographical remoteness affects babies’ risk of adverse perinatal outcomes, such as being small for gestational age and fetal death[1].
The RFDS primary care team is working to bridge this gap by providing access to best practice maternity care to those living in rural and remote communities.
“We provide face-to-face and telehealth services to women who otherwise might encounter difficulty accessing traditional maternity care due to geographic isolation,” says Mandy Smallacombe, RFDS Primary Health Care Manager.
Antenatal and postnatal services are delivered to women in outback South Australia by the RFDS Primary Health Care team, reducing the need for extensive travel for routine pregnancy care and allowing women to remain with their families and businesses until travelling to their birthing hospital in the late stage of pregnancy.
“We deliver a shared model of care between the RFDS Community Midwife, RFDS GPs and birthing hospitals in Adelaide or one of major regional centres,” explains Caitlyn Keller, RFDS Community Midwife.

The service delivers routine antenatal check-ups, blood tests, immunisations, education and support in addition to support for babies and their families once they return home after birth.
“Typically we see patients at their property or a local clinic on a fortnightly or monthly basis during regular ‘fly-in’ clinics. We are also available outside of these times for phone or video consultations,” says Caitlyn.
“Our low risk antenatal patients typically only need to travel to their birth care provider at around 20 weeks for a morphology ultrasound and consultation with an obstetrician.
“Otherwise, they can remain at home – where they often have work and family responsibilities – until much later in their pregnancy,” says Caitlyn.
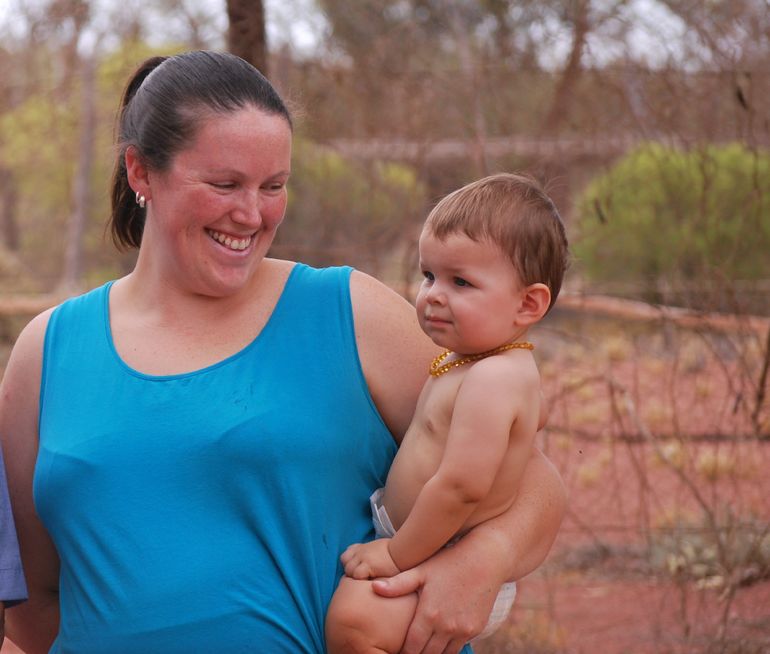
Amy Cooper is very familiar with the model of care. Amy was supported by the RFDS during her second pregnancy and is currently receiving care in her third pregnancy.
Amy and her husband live on Millers Creek Station, 150 kilometers north of Roxby Downs, SA. In addition to the busy life of a station wife, Amy supervises her children, six-year-old Riley and five-year-old Indianna with their lessons via School of the Air.
RFDS midwifery care has enabled her to stay at home until 36 weeks’ gestation.
“I see Caitlyn every month during the regular RFDS clinic run,” says Amy. “Apart from my 20 week scan, I haven’t needed to travel to Adelaide at all during my pregnancy.”
“Without the RFDS, I’d need to make a four hour round-trip on dirt roads into Roxby Downs every time I needed a check-up or blood test,” says Amy.
“It just makes everything so easy.”
The model also ensures continuity of care wherever possible. “Just like city folk, people in rural and remote areas are more likely to achieve better health outcomes when they are able to access health care from a trusted provider who understands their history and circumstance,” says Caitlyn.
“If I lived in the city, I would just see whichever midwife was on duty at the hospital at all my appointments,” says Amy. “But this way I generally see the same midwife every time, both for my antenatal care and once my baby is born.”
Did you know? Over 500 pregnant women are airlifted from rural and remote South Australia and the Northern Territory to inner-regional and city hospitals every year.
[1] Abdel-Latif ME, Bajuk B, Oei J, et al. Does rural or urban residence make a difference to neonatal outcome in premature birth? A regional study in Australia. Arch Dis Child Fetal NeonatalEd 2006; 91: F251-F256 and Roberts CL, Algert CS. The urban and rural divide for women giving birth in NSW, 1990-1997.